Paracetamol is absorbed from the gut and rapidly metabolised by the liver. A toxic metabolite is produced and glutathione is required to continue the metabolism to a safe product. Glutathione has a finite supply - if depleted the metabolite causes an acute liver injury. 4g of paracetamol is the maximum dose in a day
- ↑ AST
- ↑ PT and INR
- Falling pH
- ↑ creatinine
- normal ALP and other factors not for hepatocyte damage
N-acetylcystine dose: 150 mg/kg over 1 hour, then 50 mg/kg over 4 hours, then 100mg/kg over 16 hours
Delay in giving paracetamol due to risk of anaphylaxis when glutathione stores are not yet depleted (I believe)
Treatment pathway
Immediate to <1 hour since ingestion: Activated charcoal to prevent absorption into the bloodstream
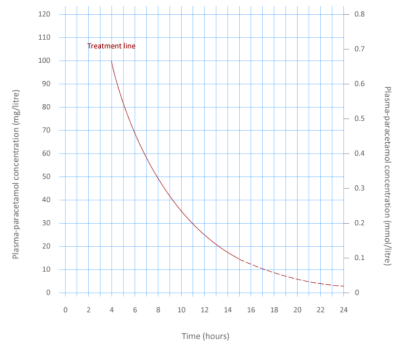
1 to 8 hours: Plot paracetamol concentration on concentration curve and determine if N-acetylcystine is required
8-24 hours: Calculate weight and start N-acetylcysteine if ingestion is > 150 mg/kg (or if paracetamol concentration is not available).
24 hours+: Start N-acetylcystine or any time if they are clearly jaundiced or have hepatic tenderness, their ALT is above the upper limit of normal
Unsure or staggered overdose: Always give N-acetylcystine if unsure of the timeline or if there was more than 1 hour between taking all of the tablets